PainRelief.com Interview with: Amnon A. Berger, MD, PhD MD/PhD Program 2006-2017 The Hebrew University Hadassah Medical School Jerusalem, Israel Resident Physician (CA-1/PGY-2) and Loring Scholar Department of Anesthesiology, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center, Boston, MA
Dr. Berger
PainRelief.com: What is the background for this study? What are the main findings?
Response: Fibromyalgia is a common disorder of chronic widespread pain. It has been estimated to affect 2-4% of the general population, though that number is likely an underestimate of the actual incidence. Outside of chronic pain, it also contributes to morbidity and disability because it affects sleep, causes cognitive impairment and psychiatric perturbations. Fibromyalgia is difficult to diagnose and even more difficult to treat.
Because the underlying causes – the etiology and pathophysiology at the base of this condition – are still largely unknown, it is harder to tailor specific treatments. There is evidence to support several modes of treatment, but truly high-level evidence exists only for physical exercise. Effective treatment depends on long term commitment and a multimodal approach by a multidisciplinary team.
Recently, with the rise of use in cannabis and CBD, both for medical and recreational use, evidence has emerged to support its use in fibromyalgia. While most of the evidence is not clear cut and not high enough evidence to support cannabis use, the evidence is overall positive and cannabis derivatives may be an effective choice as part of a multimodal treatment plan.
MedicalResearch.com Interview with: Catherine Y. Chew, PharmD, BCGP Deputy Director, Division of Drug Information Center for Drug Evaluation and Research U.S. Food and Drug Administration
Dr. Chew
MedicalResearch.com: What actions is FDA taking regarding NSAID use during pregnancy?
Response: The U.S. Food and Drug Administration (FDA) is warning that use of prescription or over-the-counter (OTC) nonsteroidal anti-inflammatory drugs (NSAIDs) from around 20 weeks of pregnancy through the end of pregnancy may cause rare but serious kidney problems in an unborn baby. This can lead to low levels of amniotic fluid surrounding the unborn baby and possible complications.
For prescription NSAIDs, FDA is requiring changes to the prescribing information to describe the risk of kidney problems in unborn babies; these kidney problems can result in low amniotic fluid. FDA is recommending that pregnant women avoid NSAIDs from around 20 weeks of pregnancy. Prescribing information already recommends avoiding NSAIDs from around 30 weeks through the end of pregnancy because NSAIDs can cause a problem that may result in heart issues in the unborn baby. If NSAID use is necessary between 20 and 30 weeks of pregnancy, NSAID use should be limited to the lowest effective dose for the shortest possible duration. Health care professionals should consider ultrasound monitoring of amniotic fluid if a pregnant woman uses NSAIDs beyond 48 hours.
FDA will also work with sponsors to request updates of the Drug Facts labels of OTC NSAIDs intended for use in adults. These labels already warn to avoid using NSAIDs during the last three months of pregnancy because the medicines may cause problems in the unborn baby or complications during delivery. The Drug Facts labels also already advise pregnant and breastfeeding women to ask a health care professional before using these medicines.
MedicalResearch.com: What did FDA find?
Response: These labeling changes are based on cases reported to FDA about low amniotic fluid levels or kidney problems in unborn babies associated with NSAID use during pregnancy. FDA’s medical literature review also contributed to the basis for the labeling changes.
Among the 35 cases of low amniotic fluid levels or kidney problems reported to FDA through 2017, all were serious. Two newborns who died had kidney failure and confirmed low amniotic fluid when mothers took NSAIDs while pregnant; three other newborns who died had kidney failure without confirmed low amniotic fluid when mothers took NSAIDs while pregnant. The low amniotic fluid levels started as early as 20 weeks of pregnancy. In 11 cases where low amniotic fluid levels were detected during pregnancy, the fluid volume returned to normal after the woman stopped taking the NSAID.
FDA’s medical literature review yielded similar findings. In these publications, low amniotic fluid levels were detected with NSAID use for varying amounts of time, ranging from 48 hours to multiple weeks. In most cases, the condition was reversible within three to six days after stopping the NSAID. In many reports, the condition was reversed when the NSAID was stopped; the condition reappeared when the same NSAID was started again.
MedicalResearch.com: What are NSAIDs? Are all NSAIDs included in the new FDA recommendations to avoid NSAID use from around 20 weeks through the end of pregnancy?
Response: For decades, people have used NSAIDs to treat pain and fever from many different long- and short-term medical conditions, such as arthritis, menstrual cramps, headaches, colds, and the flu. NSAIDs work by blocking the production of certain chemicals in the body that cause inflammation. There are both prescription and OTC NSAIDs.
NSAIDs are available alone and combined with other medicines for the temporary relief of pain and fever, including pain or fever symptoms associated with colds, flu, and insomnia. Examples of NSAIDs include ibuprofen (Advil, Motrin), naproxen (Aleve), diclofenac (Voltaren), and celecoxib (Celebrex) and aspirin.
An exception to these new FDA recommendations is the use of the low-dose aspirin (81 mg) for certain pregnancy-related conditions at any point in pregnancy under the direction of a health care professional. Low-dose aspirin may be an important treatment for some women during pregnancy. The recommendations also do not apply to NSAIDs administered directly to the eye.
MedicalResearch.com: NSAIDs already carry a warning about use in late pregnancy. What is different about these labeling changes?
Response: Warnings to avoid taking NSAIDs after about 30 weeks of pregnancy are already included in the prescribing information because taking these medications during this time may lead to heart issues in the unborn baby. The new labeling changes recommend avoiding NSAIDs as early as about 20 weeks of pregnancy because of the risk of kidney problems that result in low amniotic fluid.
MedicalResearch.com:What should pregnant women and health care professionals do? What are other options for pain relief during pregnancy?
Response: Women should not use NSAIDs after around 20 weeks in pregnancy unless specifically advised to do so by a health care professional. Because many OTC medicines contain NSAIDs, pregnant women should read the Drug Facts labels to determine if the medicines contain an NSAID. If pregnant women are unsure if a medicine contains an NSAID, they should ask a pharmacist or health care professional for help.
Other medicines, such as acetaminophen (Tylenol), are available to treat pain and fever during pregnancy. Pregnant women should ask their pharmacist or health care professional for help deciding which medication might be best.
Health care professionals should limit prescribing NSAIDs between 20 to 30 weeks of pregnancy and avoid prescribing them after 30 weeks of pregnancy. If NSAID treatment is determined necessary, health care professionals should limit use to the lowest effective dose and shortest duration possible. They should also consider ultrasound monitoring of amniotic fluid if the pregnant woman regularly uses NSAIDs longer than 48 hours and discontinue the NSAID if low amniotic fluid levels are found.
The information on MedicalResearch.com is provided for educational purposes only, and is in no way intended to diagnose, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website.
Brinda Krish, D.O., lead author of the study and an anesthesiology resident at Detroit Medical Center.
Padmavathi Patel, M.D., principal investigator of the study and Medical Director, Northstar Anesthesia at John D. Dingell Veteran Hospital.
PainRelief.com: What is the background for this study? What are the main findings?
Dr. Padmavathi Patel: Pain is a major contributor to health care costs and a common cause of long-term disability (about $61.2 billion/year) in lost productivity due to pain.
76.2 million Americans (one in four) have suffered from pain that lasts longer than 24 hours (2013).
Numerous literature such as:
1. “Use of prescription opioids in the treatment of pain has increased notably over recent decades.”
2. “Rates of death from prescribed opioids increased four fold between 2000 and 2014.”
3. “16,651 opioid related deaths in 2010.”
4. “The problem of opioid overuse and dependence is seen in the military as well as in civilian.”
-Opioid-related side effects could lead to a delay in recovery. -Pain control is more challenging for military population. -More extensive injuries and greater pain severity is seen in survivors of combat- related blast injuries compared to those of non-blast civilians and also they require larger opioid doses. -Pain is a very common patient complaint, both in veteran and non-veteran populations. -Among the 5.7 million unique patients seen annually with in the Department of Veterans Affairs (DVA), more than half of these patients experience chronic pain.
In 2017, The DVA and the United States Department of Defense (DoD) published an updated guidelines on opioid therapy for chronic pain that strongly recommends against initiation of long-term opioid use and recommends alternatives, including non-pharmacologic therapy, such as Acupuncture, which has been shown to be effective for treating a variety of painful conditions.
Acupuncture techniques have been in existence for centuries, with roots tied to Eastern Asia. Traditional acupuncture involves the insertion of very thin needles at specific trigger points around the body to relieve pain. Battlefield acupuncture (BFA), developed by a U.S. Air Force doctor uses needles that are inserted at various trigger points in the ear. In 2013, $5.4 million was awarded to the Departments of Defense and Veterans Affairs to teach BFA to healthcare providers in both the military and the Department of Veterans Affairs and assess it. In light of the opioid epidemic, there is a strong need to decrease perioperative opioid use. Opioid use due to postoperative pain along with perioperative anxiety has been linked to increased length of hospital stay, increased morbidity and mortality, and ultimately higher healthcare costs.
Battlefield acupuncture was introduced into Veterans Health Administration (VHA) in the last few years and in VHA, clinicians of various disciplines (MDs, DOs, PAs, nurse-practitioners), can currently obtain clinical privilege to provide it.
I received the Battlefield acupuncture training at John D. Dingell VA medical Center, Detroit and I was surprised with the outcomes of chronic pain patients. As an anesthesiologist I know pain after the surgery is common, often severe and largely unnecessary. I discussed these concerns with the surgeons and created the protocol to use BFA for general surgical patients and traditional acupuncture for hip replacement patients as an adjuvant to the standard protocol for acute post-surgical pain control.
Effective relief of postoperative pain is vital. Such pain probably prolongs hospital stay, as it can affect all the organ systems with side effects. Post op pain remains grossly under treated, with up to 70% of patients reporting moderate to severe pain following surgery.
Multimodal pain control not only can result in earlier discharge from hospital, but it may also reduce the onset of chronic pain syndromes.
2 studies performed TA (n=21), Controls given sham acupuncture (n=21). BFA (n=28), Controls given sham acupuncture (n=36). Measured variables included post-operative opioid requirements, postoperative pain, the incidence of PONV, and patient satisfaction scores
Key conclusions use of Battlefield acupuncture and Traditional acupuncture reduced post-operative opioid requirements, post-operative pain scores (pain intensity) and increased patient satisfaction scores. BFA also reduced PONV in patients.
PainRelief.com Interview with: Mario Moric M.S. Department of Anesthesiology Rush University Medical Center Department of Anesthesiology
PainRelief.com: What is the background for this study? What are the main findings?
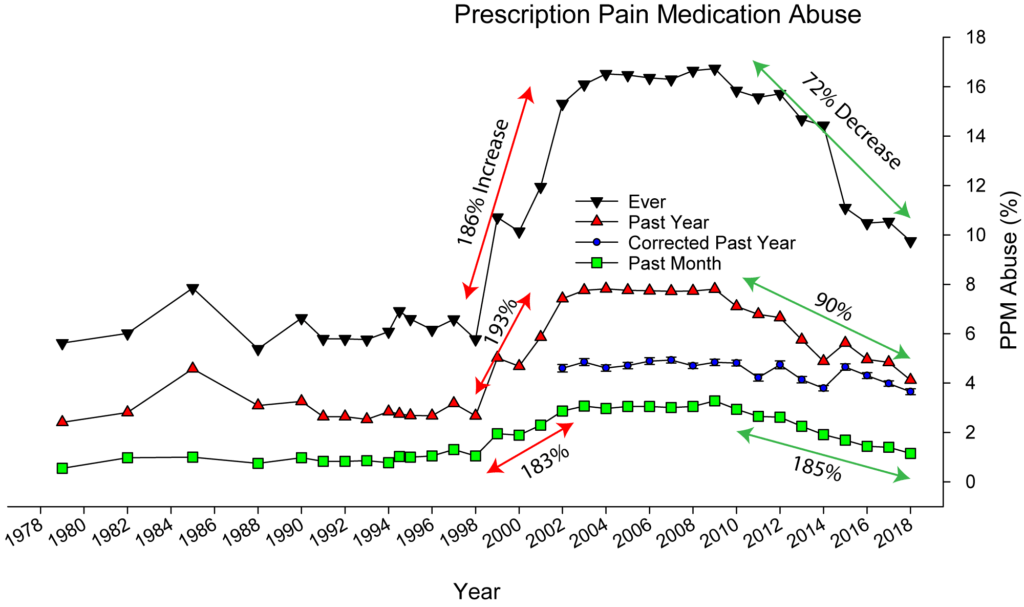
Prescription Pain Medicine (PPM) abuse has become a national problem and is now consider an epidemic. In 2012, health care providers wrote 259 million prescriptions for opioid pain medication; enough for every American adult to have a bottle of opioids.
With the recent public information campaign about the epidemic and the possible addictive nature of opioid prescription pain medications, the abuse rates have declined. We examined data from the National Survey on Drug Use and Health (NSDUH) public data derived from a national survey.
We have raw data (actual reported rates of PPM abuse, see attached image) and weighted data (corrected for the sampling design). Looking at the raw data you can see that abuse rates for lifetime use (highest line), past year use (middle red line) and past month use (bottom green line) are all more or less stable until 1998 after which we saw huge increase. From 1998 to 2004 the lifetime use increased 186%, the past year use increased 193% and the past month use increased 183%. Then the decrease, from 2009 to 2018 the lifetime use decreased 72%, the past year use decreased 90% and the past month use decreased 185%.
Using the weighted data, the past year use decreases 26% and was statistically significant, indicating a real world decrease in prescription pain medication abuse.
PainRelief.com Interview with: Rajesh Khanna, PhD Professor of Pharmacology, Anesthesiology and Neuroscience University of Arizona Tucson, AZ 85724
PainRelief.com: What is the background for this study?
Response: SARS-COV-2 infection can be spread by asymptomatic, presymptomatic, and symptomatic carriers. Transmission of SARS-CoV-2 by asymptomatic or presymptomatic individuals may account for half of the spread, which may be why the virus has been so difficult to contain. The data from our study shows that the Spike protein, the major surface antigen of SARS-CoV-2, is analgesic. Therefore, an explanation for the unabated spread may be that asymptomatic or presymptomatic individuals do not experience the pain and discomfort that act as early warning signs of infection.
PainRelief.com: What is the background for this study?
Response: Little is known about how primary care clinicians’ (PCC) approach chronic pain management in the current climate of rapidly changing guidelines and the growing body of research about risks and benefits of opioid therapy. When it comes to pain management, primary care clinicians (PCCs) find themselves in a somewhat unexpected role. Few conditions intersect with a range of specialties (i.e. mental health, orthopedics, endocrinology, etc.), disability, and aberrant behavior in the way that chronic pain does. PCCs find themselves in a position where they are asked to assess and diagnose sometimes vague and diffuse pain, and determine appropriate treatment often before the underlying cause of the pain is well-understood.
A recent cultural shift in the U.S. has created a situation in which a formerly default treatment, prescription opioid therapy, is no longer considered safe or appropriate for many patients with chronic pain. The addictive qualities and overall safety profile of opioid medications have come into sharp focus in recent years, leading to a push to reduce opioid use while also trying to achieve pain relief with little guidance for PCCs about how to manage this change in treatment plans. Others have documented the uneasiness many experience in managing patients with chronic pain. One participant in our study described the sense that opioid prescribing sometimes extends into unexpected and disconcerting territory in this way: “I never signed up to be an enforcer.” The complexity and moral uncertainty (6) associated with managing patients with chronic pain is an important backdrop for the findings from this study.
PainRelief.com Interview with: Daniel A Charen MD Leni and Peter May Department of Orthopaedic Surgery Icahn School of Medicine at Mount Sinai, New York
PainRelief.com: What is the background for this study?
Response: There is a well-established link between obesity and knee osteoarthritis, and recent research has implicated diabetes as a potential cause of cartilage degeneration. This study uses the National Health and Nutrition Examination Survey (NHANES) database to examine the association between knee pain and various metabolic factors.
PainRelief.com Interview with: Wayne B. Jonas, MD Executive Director Samueli Integrative Health Programs, H&S Ventures, Alexandria, VA
PainRelief.com: What is the background for this study?
Response: The search for non-drug approaches to chronic pain is a major recommendation in many recent guidelines for both pain management and reduction in the use of opioids. Surgical and invasive procedures are non-drug approaches often used for pain conditions like back pain and arthritis, so good evidence is needed to determine the safety and efficacy of these procedures. Properly done randomized, placebo-controlled trials are the best way (the gold standard) to get that evidence, so we did a thorough evaluation of such research, using standard systematic review and meta-analysis methods.
PainRelief.com Interview with: Md. Ataur Rahman Research Fellow Functional Materials and Microsystems Research Group School of Engineering RMIT University Melbourne, Victoria Australia
PainRelief.com: What is the background for this study?
Response: The most prevalent and critical skin receptors relate to pressure, temperature, and pain – the Pacinian corpuscle, thermoreceptor, and nociceptor, respectively. All these receptors detect stimuli, measure levels of stimuli, and transmit signals to the brain triggering reactions. The characteristic features of such human sensory system are quite complex to be mimicked by existing electronics. Development of such electronics will be a big step leading towards smart prosthetics and human-like robotics.
PainRelief.com: What are the main findings? What are some of the potential uses for this ‘skin’?
Response: While some existing technologies have used electrical signals to mimic the skin receptors, these new devices can react to real mechanical pressure, temperature, and pain, and deliver the right electronic response.
This electronic skin enable replacement of affected human skin regions, augment skin sensitivity for agile applications in defense and sports, and drive advancements in intelligent robotics.
PainRelief.com Interview with: Aliya Yakubova MD OpenLab “Gene and Cell Technologies” Institute of Fundamental Medicine, Kazan Federal University Kazan, Russia
Dr. Yakubova
PainRelief.com: What is the background for this study?
Response: Migraine is a common debilitating primary headache disorder with strong socio-economic effects. According to some estimates, migraine is the most costly neurological disease: for example, in the European Union, it costs more than 27 billion euros a year.
In this regard, chronic type of migraine (with more than 15 attacks per month for more than three months) is of special interest. Because of high prevalence and the burden of attacks, it is of great importance to improve diagnostic tools for patient stratification and choosing appropriate treatment strategies of migraine. For this purpose we investigated contribution of transient receptor potential vanilloid type 1 (TRPV1) receptors to migraine chronification. It is known that these receptors are directly involved in the disease pathogenesis being associated with the release of the key migraine pain mediator, the calcitonin gene – related peptide (CGRP). Moreover, recent studies have suggested that the non-synonymous TRPV1 single-nucleotide polymorphism (SNP) 1911A> G (rs8065080), resulting to the substitution of amino acids isoleucine to valine in the protein structure of receptor (Ile585Val), influences functional activity of these receptors in neuropathic pain syndromes. All this together was the starting point of our research in collaboration with colleagues from the University of Eastern Finland.
The information on PainRelief.com is provided for educational purposes only, and is in no way intended to diagnose, endorese, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website. None of the content on PainRelief.com is warranted by the editors or owners of PainRelief.com or Eminent Domains Inc.
Thank you for visiting PainRelief.com
Senior Editor, Marie Benz MD.
For more information, or for advertising options please email: info@MedicalResearch.com or mariebenz@yahoo.com