PainRelief.com Interview with: Sujeong Kim, PhD Institute of BioInnovation Research, Kolon Life Science Kolon One&Only Tower Seoul Korea
PainRelief.com: What is the background for this study?
Response: Neuropathic pain (NP) results from a lesion or disease affecting the somatosensory system, according to the International Association (IASP) for the Study of Pain. NP is difficult to treat and drastically influences an individual’s quality of life. Current treatment for NP aims to relieve pain and maintain patient function but does not address the etiological causes or alter the course of the condition. The causes of NP are many and varied in their scope, such as nerve injury, neuroinflammation, and abnormal pain signal transmission. NP has a multifactorial pathogenesis and their pathophysiology is the results of a very complex series of cross-linked pathway. There are limitations in treating pathogenesis by targeting only one path, so simultaneous targeting of multiple elements in NP is crucial for the treatment of the disease. Effective and disease-modifying options for NP treatment are urgently needed. We developed an AAV-based gene therapy, KLS-2031 (developed by KolonLifeScience Inc), for the expression of three therapeutic genes (encoding glutamate decarboxylase 65 (GAD65), glial cell-derived neurotrophic factor (GDNF), and interleukin 10 (IL-10)) to achieve the effective and long-lasting relief of NP.
Darwin A. Guevarra, Ph.D. Postdoctoral Fellow Michigan State University
PainRelief.com: What is the background for this study? What are the main findings?
Response:Placebos are these inactive treatments that often work because people believe they are taking a real treatment. For the most part, they have real beneficial effects. However, there’s a utility-ethical issue when it comes to placebos. On one hand, they reliably work in managing daily nonclinical nuisance like emotional distress and even a host of clinical ailments like pain and depression. But, it seems like you have to lie to people that they’re taking a real treatment in order to get placebos to work. As it turns out though, there’s over a dozen studies showing that placebos can still work even when people are fully aware they are taking them. These studies educate participants about the placebo effects, how they work, and how they can probably still work even when people know they are taking one. This really opens up the possibility of ethically harnessing the beneficial effects of placebos. But there’s one glaring issue. These studies that found positive effects of non-deceptive placebos only show it with self-report and no studies show beneficial effects on biological measures. This casts some doubt on whether these self-reported beneficial effects are real.
Our study wanted to test if we can observe non-deceptive placebo effects on objective biological markers. In this case, we used a neural measure called the late positive potential that can track emotional distress. We find that non-deceptive placebos do reduce self-reported, but more importantly, neural measures of emotional distress.
PainRelief.com Interview with: James S Thomas, PT, PhD Professor Departments of Physical Therapy and Physical Medicine and Rehabilitation Director of Motor Control Laboratory Virginia Commonwealth University Departments of Physical Therapy and Physical Medicine and Rehabilitation Director of Motor Control Laboratory Virginia Commonwealth University Richmond, VA 23298
Dr. Thomas
PainRelief.com: What is the background for this study?
Response:While there are numerous studies on spinal manipulation which is typically defined as high velocity short amplitude thrust procedure to treat a hypomobile vertebral segment, there are very few studies that examine spinal mobilization (typically described as non-thrust or as a muscle energy technique). There are even fewer studies on the comparative effectiveness of these interventions.
Accordingly, the RELIEF study was designed to provide a rigorous examination of the comparative effectiveness of the two most common manual therapy techniques for treating low back pain (i.e., manipulation versus mobilization) compared to an effective placebo (i.e., Sham Cold Laser).
PainRelief.com: What are the main findings?
Response:Relative to the placebo group, there was no difference in the change in pain or disability for either spinal manipulation or mobilization.
PainRelief.com Interview with: Dr Stephanie Mathieson PhD NHMRC Health Professional Research Early Career Fellow The University of SydneyFaculty of Medicine and Health, Sydney School of Public Health Australia
Dr Stephanie Mathieson is a Research Fellow at the Institute for Musculoskeletal Health, The University of Sydney. Her National Health and Medical Research Council (NHMRC) Health Professional Research Early Career Fellow is focused around reducing the opioid epidemic in Australia.
PainRelief.com: What is the background for this study?
Response: This study aimed to review the current evidence of the efficacy of interventions designed to reduce/cease the prescription of, or the use of, opioid analgesics in patients with chronic non-cancer pain.
As clinical practice guidelines now discourage the initial prescription of opioid analgesics for chronic non-cancer pain, clinicians need to know which opioid dose reduction methods are most effective and safe for deprescribing opioid analgesics in their patients.
PainRelief.com:? What are the main findings?
Response: Our systematic review extended the previous body of literature by incorporating five new randomised trials; however, clinical and statistical heterogeneity prevented meta-analysis. There were ten patient-focused interventions (i.e. aimed at reducing a patient’s opioid dose), and two clinician focused interventions (i.e. aimed at changing the clinician’s behaviour). Overall, our review was unable to recommend any one opioid analgesic deprescribing strategy in patients with chronic pain due to the small number of trials and heterogeneity.
PainRelief.com Interview with: Sandip Biswal MD Associate Professor of Radiology Co-Section Chief, Musculoskeletal Imaging Director, Musculoskeletal Imaging Fellowship Member, Molecular Imaging Program at Stanford (MIPS) and Bio-X Department of Radiology Stanford University School of Medicine
PainRelief.com: What is the background for this study? Response: Our ability to manage patients with chronic pain remains woefully inadequate. Chronic pain patients are faced with limited resources and inadequate care, and as a result, they make up the #1 disease group in the world—numbering more than heart disease, diabetes and cancer combined. Those suffering from low back pain, headache, fibromyalgia, arthritis and many other pain syndromes make up this ever-growing population. A big part of our inability to care for chronic pain patients is due to the fact that our current imaging methods for correctly identifying pain generators remain substantially inaccurate. Our ability to accurately identify the cause of a person’s pain, discomfort, inflammation or other related musculoskeletal symptom(s) using current clinical imaging approaches, such as magnetic resonance imaging (MRI), computed tomography (CT), digital radiography (x-ray) and ultrasound, is quite limited, lacks sensitivity/specificity and can even misguide treatment. As a musculoskeletal radiologist, I witness these shortcomings on a daily basis. I, for example, see firsthand how the lack of reliable diagnostic tools leads to significant misdiagnosis, mismanagement, incorrect use of opioids, unhelpful surgeries and, ultimately, therapeutic failures. We need a much better way to diagnose pain generators.
Accordingly, our group has been developing new clinical imaging methods that pinpoint the site of pain generation using imaging probes—more specifically, positron-emission tomography (PET) tracers that specifically target “pain receptors” or “pain molecules.” These pain receptors or pain molecules are present in abundance at the site of pain generation. After injecting one of these imaging probes into a patient through the vein, we give the probe a few minutes to circulate around the body and stick to areas that have a high density of pain receptors. We can then take a picture of the patient with a special camera that will show “hot spots” on the image that signify the location of high number of pain receptors, thereby highlighting “painful” pro-inflammatory and/or pro-nociceptive tissues. With this approach, doctors and patients have information with which they can make more objective decisions about the diagnosis and treatment of one’s pain.
Kelechi R. Okoroha, M.D. Division of Sports Medicine Department of Orthopedic Surgery Henry Ford Health System
Dr. Okoroha
PainRelief.com: What is the background for this study?
Response: The United States is in the midst of an opioid epidemic. Postoperative prescriptions following surgery is thought to have a direct role in the availability and exposure of opioids to the general population. This study was created in order to assess the viability of having common sports surgeries without the use of opioids.
PainRelief.com: What are the main findings?
Response: Our studies main findings were that common sports procedures can be performed with little or no opioids. 45% of patients did not require breakthrough opioid medication and all patients were satisfied with their pain management. Factors that were associated with requiring opioids included history of anxiety/depression.
PainRelief.com Interview with: Brian Cheng, PharmD Senior Manager, Medical Affairs Galt Pharmaceuticals
PainRelief.com: What is the background for this announcement
Response: Galt Pharmaceuticals announced a new drug approval to offer a non-opioid, non-controlled, non-addictive alternative for healthcare providers to manage patients suffering from pain. On July 8, 2020, the U.S. Food and Drug Administration approved the company’s Supplemental Abbreviated New Drug Application for Orphengesic Forte (Orphenadrine Citrate, Aspirin, Caffeine tablets 50mg/770mg/60mg), over two months ahead of the scheduled goal date.
Orphengesic Forte is indicated for the relief of mild to moderate pain of acute musculoskeletal disorders, paired with rest, physical therapy and other measures. (More Important Safety Information is below.)
PainRelief.com Interview with: Hernan Bazan, MD DFSVS FACS CEO & Co-founder, South Rampart Pharma, LLC and Professor of Surgery, Section of Vascular/Endovascular Surgery Program Director, Vascular Surgery Fellowship Ochsner Clinic New Orleans, LA 70121
Thank you for your kind invitation and opportunity to commend on our paper in press in the European Journal of Medicinal Chemistry entitled ‘A novel pipeline of 2-(benzenesulfonamide)-N-(4-hydroxyphenyl) acetamide analgesics that lack hepatotoxicity and retain antipyresis.’ This is the culmination of a multi-disciplinary effort involving investigators from the United States in Spain in search for a solution to the problem of treating pain more safely.
As a disclosure, I am the CEO and co-founder of South Rampart Pharma, LLC (https://southrampartpharma.com), which is developing its lead asset to advance the treatment of pain by developing new, small-molecule solutions that have the potential to overcome many risks associated with current pain medicines.
Dr. Hernan Bazan
PainRelief.com: What is the background for this study?
Response: The work in this paper is in large part due to several active and productive collaborations to address a simple problem: introduce a safer way to treat pain. That is, without the risk of opioids (abuse potential), acetaminophen/paracetamol (liver toxicity) and non-steroidal anti-inflammatory drugs (NSAIDs)/ibuprofen (kidney toxicity).
In 2018, over two million U.S. adults had opioid use disorder (OUD), which includes the misuse of prescription pain relievers and use of heroin (1). Prescription pain reliever misuse was the second most common form of illicit drug use in the U.S. in 2018, after marijuana use, with 3.6% of the population misusing pain relievers(1). In the U.S., pain affects more adults than diabetes and cancer combined with an estimated cost to the healthcare system of $635 billion/year(2). Current pain medications are either addictive (e.g., opioids), hepatotoxic (e.g., ApAP) or nephrotoxic (e.g., NSAIDs). For example, Paracetamol (or acetaminophen) (ApAP) is effective for acute pain but its hepatotoxicity risk limits its use to a short time period (usually < 3 days) and also its use in patients with compromised liver function or the elderly. The prevalence of OUD, including high rates of overdose in the U.S., OUD costs and toxicity profiles of currently available medications underscore the need for a safer, effective non-opioid pain medication.
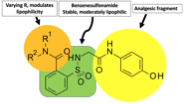
ApAP-hepatotoxicity remains the most common cause of acute liver failure in the U.S. with inadvertent hepatotoxicity the etiology in half of all cases(3). Our aim was to overcome this toxicity by creating ApAP analogs linking a saccharin moiety to the methyl group of ApAP. To this, an efficient synthesis was possible through opening the ring of the heterocyclic moiety to supply the corresponding N-substituted amides(4, 5). Within this molecule, the benzenesulfonamide fragment makes the molecule stable and moderately lipophilic and the R1 and R2 groups can be varied to effect lipophilicity (Fig).
Figure. Fragments encompassing the novel non-narcotic, 2-(benzenesulfonamide)-N-(4-hydroxyphenyl) acetamide analgesic.
This paper describes the rationale for this synthesis, the library of compounds used to select the lead compounds to develop, the consistent lack of hepatotoxicity cell lines and small animals, and its ability to reduce pain and fever in small animal studies. Moreover, we explain the mechanisms of action for the lack of hepatotoxicity.
PainRelief.com Interview with: CarrieCuttler, Ph.D. Assistant ProfessorWashington State University Department of Psychology Pullman, WA, 99164-4820
PainRelief.com: What is the background for this study?
Response: Many people report using cannabis for headache and migraine and claim that it is effective in reducing their symptoms. However, to date there has only been one clinical trial examining the effectiveness of a cannabinoid drug called Nabilone (synthetic THC that is orally administered) on headache. The results of that trial indicated that Nabilone was more effective than ibuprofen in reducing pain and increasing quality of life. There have also been a couple of preclinical (animal) studies suggesting that cannabinoids like THC may be beneficial in the treatment of migraine. But there are surprisingly few studies examining the effectiveness of cannabis, particularly whole plant cannabis rather than synthetic cannabinoids on headache and migraine.
Donald I. Abrams, MD Division of Hematology-Oncology Department of Medicine, Zuckerberg San Francisco General Hospital University of California, San Francisco
PainRelief.com: What is the background for this study? What are the main findings?
Response: A number of years ago, Kalpna Gupta, PhD, an investigator then at the University of Minnesota, came and told me about her mice with Hemoglobin SS who experienced pain that responded to laboratory cannabinoids. She was going to apply for a grant from the National Heart, Lung and Blood Institute to continue her studies and sought us out because of our prior clinical trials with cannabis and pain. Dr. Gupta wanted to include a pilot proof of principle human study in her application and asked if we could design one. As cannabidiol (CBD) was just becoming known at that time, we suggested to do a study in patients with sickle cell disease and pain looking at a delta-9-tetrahydrocannabinol (THC)-dominant strain of inhaled cannabis, a CBD-dominant strain, a balanced 1:1 strain and placebo. She said that we would only have funds to do a two-arm study, one of which needed to be placebo. As we had already shown that there was a trend for vaporized cannabis that was predominantly THC to add to the analgesic effect of sustained-release opioids in patients with chronic pain, we chose to investigate a 4.4% THC:4.9% CBD product obtained from the National Institute on Drug Abuse.
We designed a crossover trial so that each participant would spend two 5-day inpatient stays separated by at least a month in our Clinical Research Center at Zuckerberg San Francisco General Hospital. During one stay they would add vaporized cannabis to their stable ongoing analgesic regimen and during the other stay they would inhale placebo cannabis three times a day. We use the Volcano vaporizer device that heats the plant material and not an oil as has become popular in the recent “vaping” craze. Our target was to enroll 35 patients with sickle cell disease and chronic ongoing pain on an opioid-containing regimen. Our primary endpoint was change in pain as measured by way of a visual analog scale and the Brief Pain Inventory as well as safety.
The information on PainRelief.com is provided for educational purposes only, and is in no way intended to diagnose, endorese, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website. None of the content on PainRelief.com is warranted by the editors or owners of PainRelief.com or Eminent Domains Inc.
Thank you for visiting PainRelief.com
Senior Editor, Marie Benz MD.
For more information, or for advertising options please email: [email protected] or [email protected]